RECENTLY PUBLISHED ARTICLE
A Cutting–Edge brain surgery for tremore, without surgery
Surgeons are using focused ultrasound waves to treat essential tremor.
It might help people with Parkinson's, brain cancer, and even ALS.
Boston Globe Sunday Magazine, 11/27/2019 cover.
By Mark Kramer
Lou Pandolfe looks at his freshly shaved scalp in a mirror and smiles ruefully at the unfamiliar reflection smiling back. The previous evening, he and his wife, Christine, drove up to Boston from their home in West Hartford, Connecticut, for pre-op preceding a new type of brain surgery at Brigham and Women’s Hospital. Tomorrow, Pandolfe will turn 77. He and Christine hope a successful surgery will be his birthday gift.
Over the last two decades, Pandolfe developed a serious tremor of his limbs and his voice. His shaking got so severe he often had to stop what he was doing when he still worked at the auto parts company his father had started as a scrap yard during the Great Depression. “I was struggling with handwriting and working with equipment,” he says. “The guys in the shop couldn’t read my work orders.” Navigating a screwdriver into a screwhead took grim concentration, fighting the tremor and gripping the tool with both hands. He’d enjoyed singing but his voice has diminished to a growly tremolo. He can’t raise a glass of water to his lips without sloshing it on himself.
Except for the tremor, Pandolfe is pretty healthy, with a daughter and son he visits, and grandkids who love to play with him. “I never felt embarrassed by the tremor,” he says. But he longs to have his hands, voice, and sense of control back. A few years ago, a neurologist told him he had something called “benign essential tremor,” a condition involving a disruption in the thalamus, a relay point in the brain for touch, pain, and other sensations. This type of tremor afflicts 7 million to 10 million Americans, and Pandolfe is in the 10 percent suffering severe symptoms.
His neurosurgeon, Dr. Rees Cosgrove, stands beside him in the white-walled prep room, surgical suite L1, bay 3 at the Brigham. Cosgrove gently encircles Pandolfe’s bald, shining head at hat-brim level with a gray metal frame about an inch wide. He peels and refastens the Velcro webbing supporting it, until it hangs evenly just above Pandolfe’s eyebrows.
Cosgrove and a neurosurgical resident poke long needles of novocaine through holes in the front and back of the frame. Then they insert and tighten bolts with sharp tips that dig in to the skull and stop the frame from slipping. Pandolfe winces. “That was the worst part of your day,” Cosgrove says. “Does the frame feel tight?”
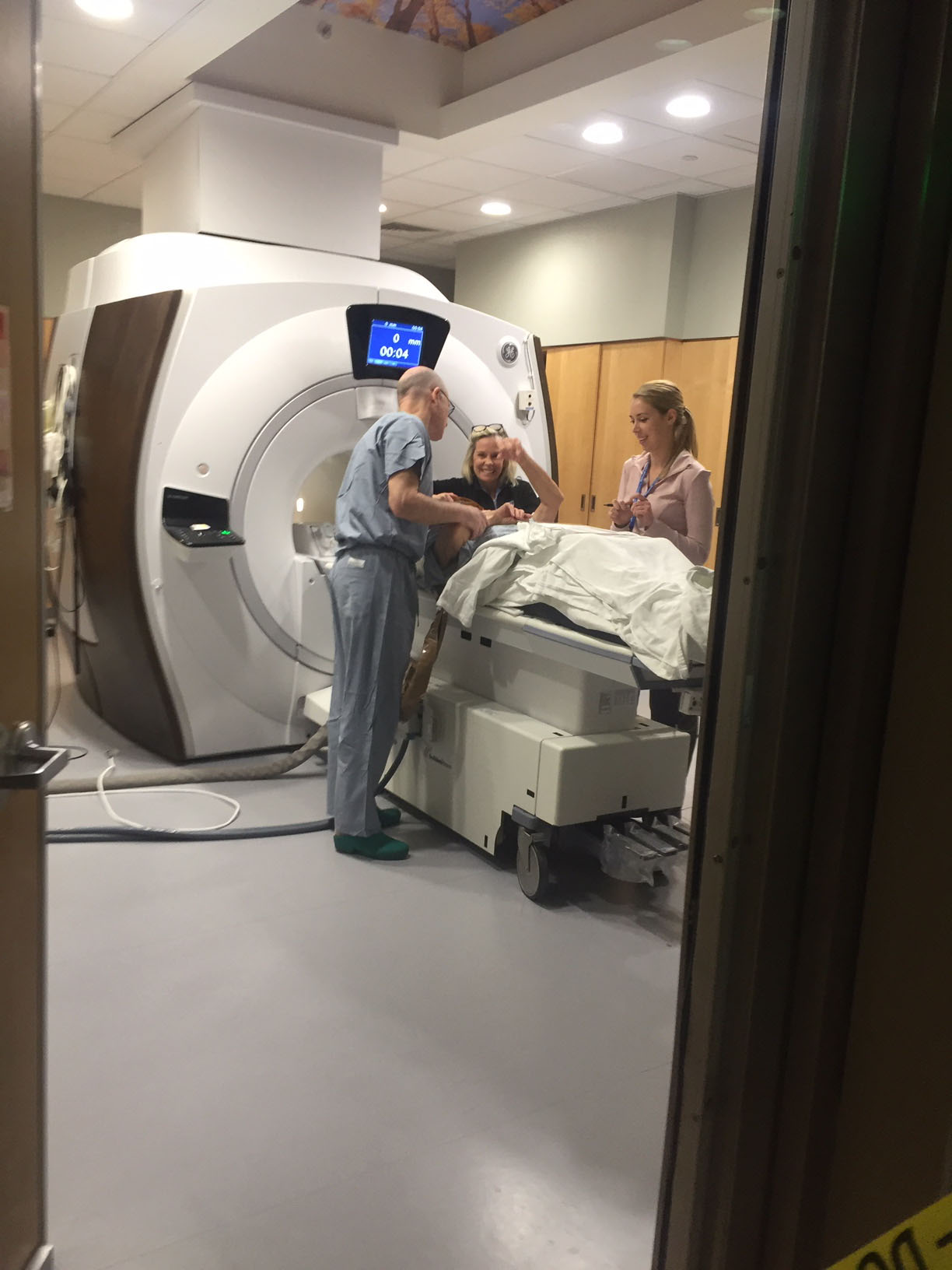
Pandolfe, tall, gangly, and quiet, not sedated at all, stands up from the prep chair and follows Cosgrove and his physician’s assistant, Sarah Christie, into the next room. They help Pandolfe lie, face up, on a gurney that will slide into a huge MRI machine. Then they wrestle a gasket-tight hat — it looks like a pith helmet designed by Salvador Dalí — over the top of his skull. After it’s securely sealed, the team clamps Pandolfe’s rubber-hatted head to the gurney, then lowers a double-walled dome like a beauty-parlor hair dryer on top of the frame. They fill the dome with water.
For the next two hours of precision brain mapping and fastidious surgery, the patient’s head must not even wiggle. Cosgrove and his team will focus ultrasound waves on a spot deep in Pandolfe’s brain, burning up part of the circuitry of his tremor. Pandolfe’s head is bolted down because a millimeter or two shift could burn the wrong part of the brain, which might slur speech, numb a hand, or leave him with weakened limbs, imbalance, even cognitive difficulties.
Before settling on this new surgery, Pandolfe had looked into his options. Since medication wasn’t working for him — “it made me dizzy,” he says — deep brain stimulation was the standard approach. That procedure involves drilling burr holes in the skull, inserting wire-thin electrodes into both thalami, and linking them to a neural pacemaker implanted in the patient’s chest. This eases tremor in both arms, but it is costly, there is a risk of infection, and the pacemaker batteries must be surgically replaced every two years. Pandolfe thought it seemed too complicated.
One of Pandolfe’s neurologists knew of the new procedure being performed by Cosgrove at Brigham and Women’s. Cosgrove is soft-spoken, 62, with three grown daughters. He’s done his share of deep brain stimulation surgeries. He has about the same tall, thin build as Pandolfe, and he too was born to his vocation. “It chose me,” he says. His father, a neurologist at Montreal Neurological Institute, was also “a concert-quality pianist who loved Mozart. I prefer Bach.”
Cosgrove met with the Pandolfes and told them more about the new approach, that it took just a few hours, and that it did not involve cutting into the patient or a pacemaker. And, best of all, the relief it offered from tremors appeared to be permanent. Pandolfe met the obvious requirements: He was over 21, and his tremor interfered with his life and did not respond well to medication. After the meeting, Pandolfe felt certain: He would do the surgery.
Essential tremor is the first condition the Food and Drug Administration has approved for noninvasive surgery with focused ultrasound, the formal term for the treatment Pandolfe is undergoing. Rees Cosgrove is the only person performing it in New England — Pandolfe is the 53rd person he’ll operate on. The procedure is the cumulative result of decades of big science, research started here at the Brigham, major studies, published papers, and clinical trials funded by foundations, government grants, and big businesses. A company called Insightec accumulated the intellectual property, undertook further research, and commercialized the process.
In December 2018, focused ultrasound treatment for Parkinson’s with tremor was also approved by the FDA. Treatments of other forms of Parkinson’s are in various stages of study; movement disorders are among the biggest potential applications of the new technology. The company is also evaluating neuro-oncology — Insightec is developing a trial for glioblastoma, a form of brain cancer. A third area of possibility is neurodegenerative diseases such as Alzheimer’s, amyotrophic lateral sclerosis (ALS), and some types of obsessive compulsive disorder, although the company’s CEO and chairman, Maurice Ferré, says that “it’s too early to see if we’ll have an impact.”
Ferré, whose father served six terms as mayor of Miami, says the company is in “the first or second inning” in terms of its market potential. Insightec, based in Haifa, Israel, and Miami, has raised nearly $400 million in venture capital from investors such as GE Healthcare, York Capital Management, and Koch Industries’ Koch Disruptive Technologies fund.
The procedure itself has roots in Brigham research that goes back to the 1980s, under the late Dr. Ferenc Jolesz, a pioneering neurosurgeon and radiology researcher. Some four decades on, the technology is seeing hopeful early results. Although it’s hard to call something a breakthrough that is still breaking through, but focused ultrasound is attention-getting.
Pandolfe lies in the mouth of the MRI. Cosgrove holds a clipboard above Pandolfe’s chest and asks him to reach upward and draw first a spiral, then a straight line, with only the pen touching the paper. Pandolfe, arms shaky, produces a tangle of lines with little relationship to a spiral. The straight line comes out as jagged as an electrocardiogram. “This gives us a baseline,” Cosgrove tells him.
The double-walled, water-filled helmet is one of the main innovations enabling this new surgery. Ultrasound waves penetrate the skull without damaging the brain; the inside of the helmet is studded with 1,025 tiny ultrasound emitters that converge the waves on a target in the brain the way a magnifying glass concentrates sunlight to sear a hole in a leaf. (About 15 percent of skulls are too thick for this surgery.)
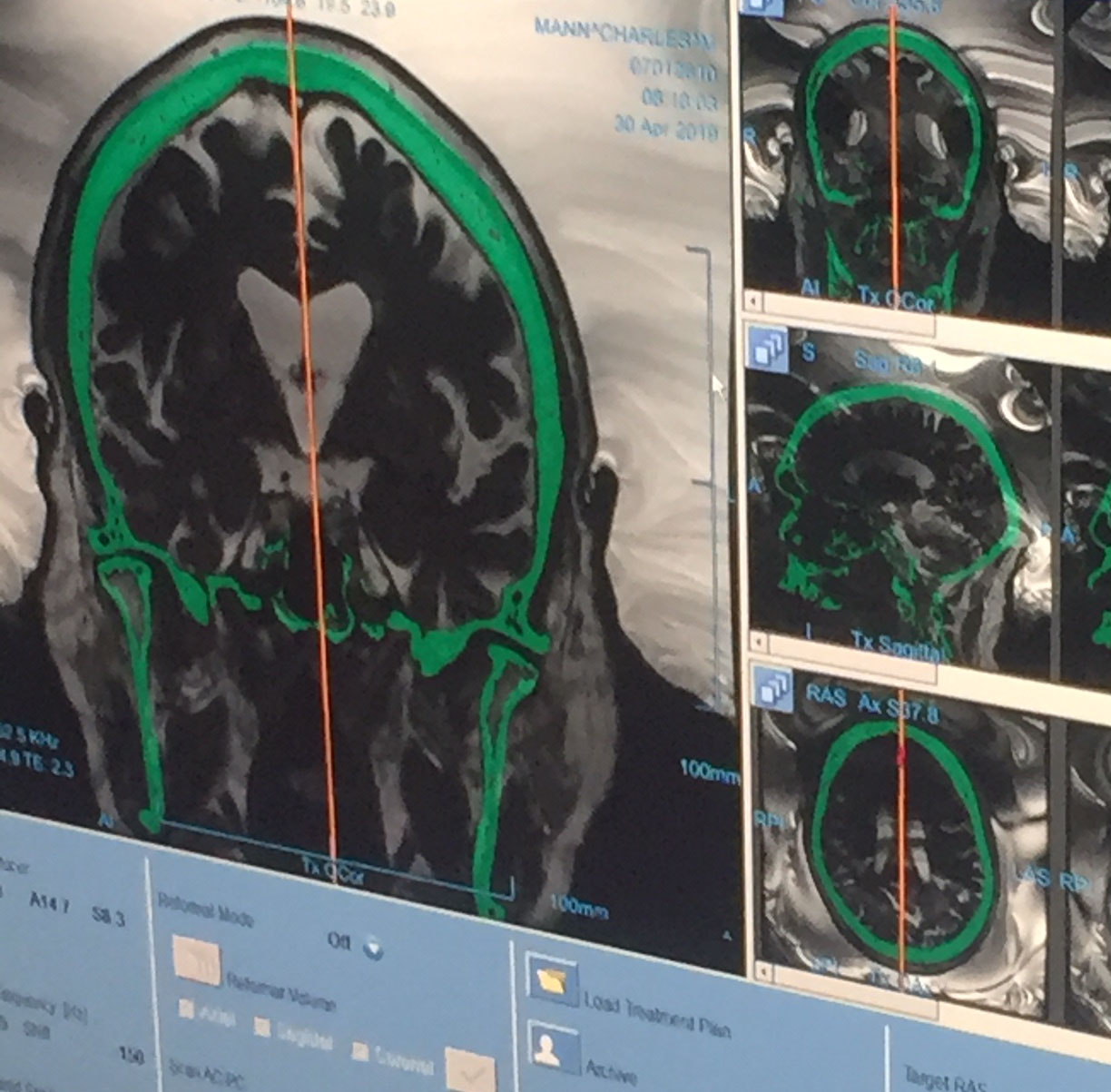
The left and right thalami are walnut-shaped clusters in the middle of the brain involved with perception, consciousness, strength, emotion, and sensation. The new technology precisely locates a lobe in the thalamus about the size of a pencil eraser, called the ventrolateral nucleus, and then ablates (medical parlance for sizzles) a part of it, reducing or relieving the tremor.
Cosgrove will destroy, incrementally, a quarter-of-an-inch sphere inside Pandolfe’s left thalamus.
Pandolfe is still lying in the MRI machine an hour later, alone in the big room. The crew has loaded in his previous CAT scan and integrated it with his real-time MRI scan. In the adjacent control corridor, Cosgrove and a surgical team meticulously locate their target, specifying its coordinates to half a millimeter. The surgeon will be a pilot feeling his way toward a fogged-in landing with his instruments guiding him: He’ll depend on the images and data on the computer screens that sit on a long counter jumbled with wires.
The crew, all 11 of them, have been doing these operations for two years now. Their tasks are familiar. A nurse, an MRI tech, and the physician’s assistant have set roles monitoring and tending to the patient and the equipment. To Cosgrove’s right sits a PhD ultrasound physicist, Jason White. To White’s right sits a senior engineer for Insightec. They trade quips and also technical information. Some sit at keyboards and some stand, peering at the screens and meters, and, occasionally, in at the patient.
A few rubbernecking neurology residents and medical students squeeze against the far wall of the corridor, drawn by word of the goings-on. Also here are three senior sales representatives from Insightec: the Brigham account representative, the East Coast sales manager, and their new boss.
“It’s the happiest operating room in the Brigham,” says Cosgrove, joking with surprising sociability for someone about to perform surgery. The physicist at the MRI screen flips through cross-sections of Pandolfe’s brain. Image resolution has become crisper — a critical innovation but not as new as the helmet and the software integrating images and controlling the ultrasound beams.
Cosgrove scans the anatomy, shadows, and glowing patches that resolve into familiar brain structures he’s so often visited in open-skull surgery. He studies the images from several directions, the shadows of the thalamus. He double-checks the critical adjacent structures he must leave undamaged at all costs.
Most operations are termed invasive procedures, and they do each commence with a visible invasion: A scalpel slices skin. Noninvasive procedures start far less dramatically. Cosgrove clicks on a mike and says, “OK, Lou, we’re starting now.”
The physicist finally clicks the little button labeled “sonicate” in the left corner of the screen. After 20 seconds of processing time, the whirring from the next room gets louder. This first pulse is low-intensity — just enough to warm the target area. A graph line on the computer screen spikes upward, toward 50 degrees Celsius, 122 Fahrenheit, stays level through 1 . . . 2 . . . 3 . . . 4 . . . 5 . . . seconds, and then drops.
Cosgrove and the nurses spring from their seats, rush into the MRI room and determine in seconds, as the gurney slides out of the machine, that Pandolfe isn’t nauseated. The procedure can cause vomiting, a danger for the immobilized patient.
Pandolfe looks up at them. Cosgrove asks him to say a test phrase: “I took a train to Topeka, Kansas.” The T’s show when the tip of the tongue starts to be affected, the K’s, the back of the tongue. Slightly slurred speech is a sign that the surgery has gone far enough. He touches Pandolfe’s lips and fingers.
“Lou, how did that feel?” Cosgrove asks.
“That didn’t bother me. I felt a little spinning,” Pandolfe answers.
The dose has been light, so they don’t expect much tingling yet, just enough to show they’re on target.
Pandolfe is slid back into the machine. Cosgrove leaves, followed by the crew. And soon Cosgrove says into the patient’s earphones, “Lou, we’re going to do it again — a little stronger.”
The physicist again clicks the sonicate button on his computer screen. Ten seconds later the temperature graph reads 60 degrees Celsius — up to 144 degrees Fahrenheit. The MRI buzzes loudly. A small ketchup-red splotch appears near the center of Pandolfe’s brain image on the computer monitor. It’s the beginning of the ablated area.
Cosgrove and the crew again rush in to Pandolfe. Cosgrove holds up the clipboard again and, speaking louder and enunciating, asks him to please reach up and draw another spiral and another line. The spiral this time is recognizable, if shaky. The line is still spikes and valleys, but shallower. They ask him to hold his arms up above his chest, then point his index fingers at each other without letting them touch. His arms flap about, as though he’s conducting an orchestra still tuning up. The finger-touching exercise demonstrates the state of the tremor.
The crew zaps Pandolfe five more times, punctuated by trots in to see him, improving spirals and lines, more trains to Topeka. With each round of ultrasound, the ketchup-colored ball expands a little on the screen.
“I felt like I was going backwards, head first, down a roller coaster,” Pandolfe will recall. “It wasn’t pain, but I don’t like heights. I was more daring when I was young. It increased every time. The heat was almost like a shock. I could see I was improving each time I drew a spiral — that was a big incentive to keep going.”
After the seventh zap, Pandolfe’s right arm barely shakes when his gurney rolls out of the MRI machine. He draws a presentable spiral and a good line. His right hand has stopped conducting. Since the procedure only fixes one side (patient’s choice), his left arm still shakes. His right arm and hand are all but still — a slight tremor persists in his right wrist. On the screen the irregular red circle glows larger, the destroyed hole in the thalamus, widened with each zap, nearing the dangerous off-limits zone.
Cosgrove ponders. Should he try one more round? If the tissue doesn’t reach a certain temperature, the neurons won’t be killed, and the tremor could return. But there’s the risk of permanently slurred speech, weak muscles, foggy thinking, or worse. Cosgrove says he feels both the pull toward caution and the desire to do a thorough job. “Above all, do no harm,” he says.
He asks the physicist for various views of the lesion. Cosgrove studies for a full five minutes, saying nothing. Perhaps he is wrestling with detachment from his own wish to get things just right, weighing scientific considerations and odds. He has performed brain surgeries for decades, invasively. He knows the map and which interventions provoke which responses.
Observing Pandolfe’s surgery is awe-inspiring — so much costly research and skilled care and expensive machinery and facility time poured into making an already quite happy middle-class life even better. But it raises another question: Who should have access to this life-altering technology? Insightec won’t say what this procedure will cost as it spreads, but right now the average Medicare reimbursement seems to be about $12,500.
A part of Medicare, though, is expected to go bankrupt in 2026, says Jonathan Gruber, a health economist at MIT. He adds that a new, promising procedure that drives high demand may “just hasten bankruptcy.” That could leave it as something the rich will get most easily, barring an unexpected shift in US policies on taxation and health care regulation.
The question of how the United States allocates, or fails to allocate, health care spending is not Cosgrove’s concern. He has reached one of those low-odds-of-failure, high-consequences-for-failing moments. He has taken the time, and finally says, almost to himself, “Perfection is the enemy of good,” a guideline he first heard from one of his mentors. No additional zap. The crew trots in and unlatches the water-filled dome. They peel the rubber gasket off Pandolfe’s head and a nurse throws it in the surgical waste pail.
Pandolfe looks beat up. He sits up on the bench, then stands, and then walks gingerly through two rooms and down a long hallway. A nurse and the PA hover to catch him if he suffers the weakness patients sometimes have. But he stays on his feet, and eases onto a bed in the recovery room. The nurse hands him a cup of water. He grasps it easily with his right hand and sips. Christine, Lou’s wife, touches his hand as he drinks, as if making sure it really has quieted.
A week later, he’s still marveling. “They told me to take a drink — and I did. I was more than elated. It was amazing to look at my hand holding the cup and say, ‘I can do this.’ I don’t believe in miracles. But this seemed like a miracle.”
Three months later, Pandolfe is still amazed. “I still check it every morning,” he says. He and his wife have again driven to the Brigham, where he’s had a follow-up MRI. Cosgrove examines the images in his office with them. He’s called in Dr. Michael Hayes, the original referring neurologist, to see his handiwork.
The brain lesion Cosgrove had made has healed — the tremor in the right arm is nearly gone and doctors expect it will stay that way. Pandolfe says he feels relieved. His wife, realizing he’s got two experts looking through the images of his brain, in a moment of daring asks, “Do you see any signs of Alzheimer’s?” Both doctors, smiling, tell her no.
Mark Kramer is a journalist and author in Newton. He founded the Nieman Foundation program on narrative journalism at Harvard, and runs narrative writing conferences in many countries. Send comments to magazine@globe.com.